
Thoughts on Martin Luther King Day
{NOTE: This is a slightly-edited reprint of a previous post.]
I have some trouble with the hagiography of Martin Luther King. I agree that he was a great man who did a great thing for which he should be duly honored: he was an inspirational figure in the non-violent civil rights movement in this country, as well as a remarkable speaker.
The two, of course, are related. It was his personal quality of leadership, and what George H.W. Bush might rightly call “the vision thing,” that enabled King to bring together so many people to peacefully demonstrate in furtherance of a lofty and necessary goal, that of ending discrimination against blacks in this country.
As for the rest of it—well, I think it can be summed up by saying that King was a flawed human being—that is, a human being. Perhaps MLK himself would be the first to agree; he was a preacher, after all, and he knew a lot about human sin and error. It’s pretty much certain he was a philanderer as well as a plagiarist, and in later life he seemed to veer ever more leftward (some think that’s a feature, not a bug).
Does that diminish his achievements? I don’t think so, if we keep it in perspective. I’ve always been more interested in real human beings who accomplish great things despite their own weaknesses than I am in a pretended (and mostly unachievable) perfection.
[NOTE: One thing that’s long amazed me is that King was so young when he was assassinated. At the time I thought him a man in his 50s, but he was actually a mere 39 years old. If he were alive today, he would only have just turned 85 yesterday.
There’s a lot of speculation on what King would have thought of current trends had he lived. I’m no expert on everything the man wrote and said, but it’s my impression that although he seemed to be in favor of some sort of reparations—which he did not limit to blacks, by the way—he would not have backed affirmative action or gay marriage. However, people do change—as I know only too well.]
Obama and those racist “folks”
Actually, compared to a lot of ways that Obama and his supporters have used the race card, this is relatively mild and balanced:
There’s no doubt that there’s some folks who just really dislike me because they don’t like the idea of a black president,” Obama said in the article by David Remnick, appearing in [The New Yorker’s] Jan. 27 edition.
“Now, the flip side of it is there are some black folks and maybe some white folks who really like me and give me the benefit of the doubt precisely because I’m a black president,” Obama said in his most direct comments on how race has affected his political standing since he’s been in office.
If you just look at the literal meaning of what Obama said, it’s certainly true. As a writer, I’ve often noticed people’s word choices, and that word “some” is especially useful. It means anything from one or two to many, and is almost always true, although not especially informative about numbers. As such, it’s a dodgy, safe word.
In other words, I have no doubt that there are some people (Obama likes to use “folks” when he’s feeling especially proletarian and wants to sound—folksy) who “really dislike” him “because they don’t like the idea of a black president.” I happen not to think they are especially numerous in terms of percentages of the populace, but to deny that “some” exist would be absurd. And although it’s rare for him to acknowledge the other side, which is that there are “some black folks and maybe some white folks who really like me and give me the benefit of the doubt precisely because I’m a black president,” that statement is also undeniably true. In the latter case, the “some” is probably “many,”—more than the number who dislike him because he’s black.
Most of the anti-Obama racists probably don’t dislike him only because he’s black, of course. There are plenty of other reasons to dislike him. And most of the people who “dislike” him don’t care if he’s black, yellow, white, pink, brown, or green, but “dislike” him because they are against his policies and his power grabs, as well as his divisive rhetoric and his lies. There are even “some” people (and I believe they are very numerous) who detest him and his policies but were originally predisposed to like him and give him the benefit of the doubt because he’s black, but over time he’s worn down their goodwill and now they have no doubt and therefore no benefit to give him anymore.
So, what’s Obama doing in the above statement? Well, it’s a version of something he likes to do quite a bit, which is to bring up a topic such as race in a way that sounds reasonable on the face of it but is actually a call to his supporters to use what he says in a different way: i.e. to continue with their incessant charges that dislike of Obama’s policies is grounded in anti-black racism. He has never to my knowledge spoken out against those who make that charge, and he’s been encouraging them to do so in ways both subtle and un- ever since his campaign in 2008.
I described the phenomenon in some detail in this post from July of 2008. But perhaps the best quote to show you how early Obama was doing this and how basic it was to his campaign is from this post written in June of 2008, which I believe is the first time I remarked on it. It’s not a very long post, so I’ll just repeat it here in its entirety:
Barack Obama, the candidate who wants to end divisiveness, and who wants to run a clean and honorable campaign without negativity, said the following in a recent campaign speech at a Florida fund-raising reception:
“It is going to be very difficult for Republicans to run on their stewardship of the economy or their outstanding foreign policy. We know what kind of campaign they’re going to run. They’re going to try to make you afraid. They’re going to try to make you afraid of me. He’s young and inexperienced and he’s got a funny name. And did I mention he’s black?”
We have here a truly masterful attempt to flames of paranoia on the part of his followers and adopt the mantle of victimization for himself, thus raising rather than lowering the amount of divisiveness and vitriol in the campaign. Pretty good for just a couple of sentences.
Obama is correct in saying that there have been racist remarks against him. These have originated from fringe elements and/or commenters in the blogosphere and/or anonymous email campaigns. They focus on his “funny name,” for example, or the fact that he’s black.
But in this speech he appears to attribute””or to encourage his supporters to attribute””these charges to the entire Republican Party, couched as a threatening “they.” At the same time, he fails to differentiate these attacks””and actually connects them as part of an undifferentiated list””from extremely legitimate concerns that people have voiced about other characteristics of his, such as his inexperience.
In the final sentence of the paragraph he slyly encourages a phenomenon I’ve noticed happening more and more: the charge that any criticism of Obama emanates from racism. If the racism isn’t overt and clear, as in the emails, then it’s covert; “inexperience” (a valid concern based on the objective facts of his history) becomes a code word (wink wink) for hidden racism and fearmongering.
This is dangerous demagoguery.
Because one so seldom hears overt expressions of racism any more, and certainly not from mainstream candidates, there has been a tendency to imagine it is everywhere, but hidden. Here Obama cynically fosters that belief and encourages the definition of his entire opposition as energized by this impossible-to-prove””or, more importantly, impossible-to-disprove””motive.
No, it turns out that most of them haven’t mentioned he’s black, except in approving terms. But they don’t have to nowadays to be racists; Obama has taken care of that.
Speaking of giving Obama the benefit of the doubt—I continue to be astounded, looking back at 2008, that more people didn’t see the perniciousness of what he was doing at the time regarding race. Compared to what Obama was saying in 2008, his remarks to Remnick were mild. He can afford to be mild now because the damage has been done. The meme he planted so firmly in 2008 has borne tremendous fruit in terms of helping him get re-elected, and helping to further racial tensions in this country rather than dampen them down.
[NOTE: By the way, I’m tired of people writing that the fact that Obama’s support from black people is 90+ percent is evidence of blacks’ pro-Obama racism because he’s a black man. Although it is almost certainly the case that blacks are extra-reluctant to abandon Obama, and that being black only enhances his support from blacks, the percentages of black people supporting Obama are not so very much higher than the percentages of black people supporting other recent Democratic presidents (or presidential candidates) such as Clinton or Gore or even Kerry. In fact, if you look at the following chart, you’ll see that ever since the New Deal blacks have been quite solid in their support of Democratic presidential candidates, a support that went even higher after the passage of the Civil Rights Act during the 60s:
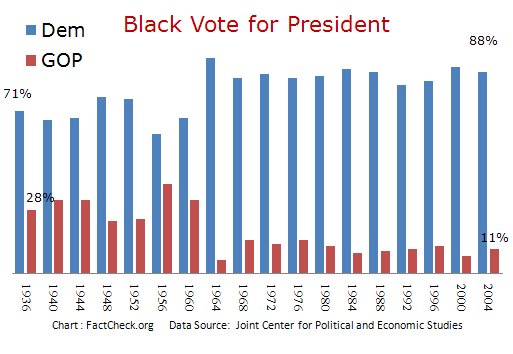
What’s more, in recent years, even white Democrat candidates such as Clinton, Gore,and Kerry all lost the white vote, just as Obama did. If you want some mind-blowing statistics, take a look:
Add Obama’s name to a long list of white Democrats who lost that demographic: Humphrey in 1968; McGovern in 1972; Carter in 1976 and 1980; Mondale in 1984; Dukakis in 1988; Clinton in 1992 and 1996; Gore in 2000.
In fact, white voters preferred Obama to Sen. John Kerry ”” who lost the white vote by 17 points in 2004, while Obama lost it in 2008 by “only” 12 points. Obama improved on Kerry’s share of the white vote in every age demographic, including the 18- to 29-year-olds (which Kerry lost).
The truth is that minorities such as blacks constitute the margin of victory for Democratic candidates, black or white, on the national level, and this has been true for quite some time. The racial divide is not mostly about the race of the candidate, although it has a role. It is about the party affiliation of the candidate and the party affiliation of the members of the different races, and how differently the parties are perceived in terms of philosophy and action, including how each party affects each race. The irony, of course, is that black people have done poorly under Obama’s watch, and under the welfare state as a whole.
Thomas Sowell wrote the book (literally) on this. Here’s a small snippet of his thoughts.]
Separated at birth
These two really were separated at birth.
Literally.



Republicans: why can’t we all get along?
Trying to get Republicans to agree on something is like herding cats. Democrats tend to hang together for the good of the Party and the larger vision, as well as the promise of more specific rewards for cooperation (jobs, pork, etc.) or threats for non-cooperation. But Republican seem a lot more disorganized—or is it ornery or individualistic or uncompromising or principled or stupid or what?
I was thinking about that yesterday, and I thought the issue might deserve highlighting in a thread of its own:
I was watching some commentator on some TV news show on Fox (forget who) saying that Republicans had a lot of Obamacare-alternative proposals but needed to get together and settle on one to get behind…What is up with this stupid inability to come together? I think it’s the lack of the ability to compromise with each other that I was talking about the other day.
Note that here I’m not talking about, nor suggesting, compromise with the Democrats. I’m talking about presenting a united face to the public so that the message of the right is clear and understandable, and something people can relate to. And then to drive it home with repetition and memorable phrases.
Scott Walker had some good things to say in his interview with John Hawkins, which I quoted yesterday:
…the Left, they want you under their thumb. They want to control you. They want to control your lives. They want you to be dependent on the government. We should say we’re the ones, not only for the poor, but for young people coming out of college, for working class families, for immigrants, for others out there. We should say we are the ones who empower the American Dream. We’re the ones who say you can do and be anything you want, but it’s because we empower you with the ability and the platform to do that.
Now, is that so hard to say? Apparently.
In the years I’ve been on the right, I’ve been impressed by how much infighting there is compared to the left. Not that the left doesn’t have disagreements, but they pull together for the sake of the all-important prize: winning. Conservatives seems to take pride in their dissent from each other, as though it shows their integrity and their devotion to principle.
And I suppose in a way it does. But as a strategy (or is that a tactic?) it stinks.
Impeaching Obama
On a Hot Air thread about the desirability of impeaching Obama I saw this comment:
Impeachment would be like a child throwing a temper tantrum ”” lots of sound and fury signifying extreme frustration. But in the end Obama would still be there. I know futile gestures that antagonize the unengaged electorate are satisfying to the Kamikaze brigade but a bound to fail impeachment attempt would all but destroy the Republican chances to take the Senate and make gains in the House. If you want to do something to reign in Obama then I suggest if you are dissatisfied by your current Republican member of Congress vote for his opponent in the primary but if you lose show up November to vote (R). Failure to do so provides aid and comfort to Obama’s socialist agenda.
And this:
George Will wrote about “gesture liberalism” last week. There is such a thing as “gesture conservatism” too, and proponents of impeachment are its chief practitioners. They tend to share with liberals the notion that the main goal of politics is to make them feel good, and righteous. It isn’t.
I would not say impeachment is an absolute impossibility before Obama’s second term is through. But impeachment would be a very bad idea at this point, even though the GOP controls the House, and even though there’s plenty of fodder for impeachment.
For the sake of argument let’s say the Republicans in the House have the guts and the votes to do it. But the effort can go nowhere in the Senate—they will not get the requisite two-thirds for conviction—and would only anger the public, the great majority of whom would find it to be vindictive overkill (as well as something that gets in the way of whatever it is that they think Congress is supposed to be doing instead). Such an action would increase Obama’s approval rating, and perhaps even lead to the Democrats holding the Senate or even making advances in both bodies of Congress.
However, if Obamacare goes forward and things get worse, and the Republicans win the Senate in 2014 (even if they don’t get over 2/3 of the seats there, which they almost certainly won’t), and Obama’s approval ratings drop into the cellar (low 30s or less), then there’s a chance. The public might get behind impeachment/conviction, and it’s theoretically possible (although unlikely) that even a few Democrats might come along.
That’s the only way it could happen, and I give it an infinitesimally small chance of coming about. But one thing is certain: now is most definitely not the time for impeachment. Ralph Waldo Emerson is reputed to have said, “When you strike at a king, you must kill him.” He was supposed to have been responding to a student “who had told Emerson that he was writing an essay about, and presumably critical of, Plato.” Emerson wasn’t talking about literally killing Plato, who had been dead for quite some time. He was talking about knowing how to chose the right time and way to undermine a person regarded as a great and powerful man.
The same is true of impeaching Obama: don’t start unless you have the votes in the Senate to convict, and the support of the American people, or you will end up hurting yourself. Impeachment has legal trappings, but its essence is political. So whether Obama has committed an impeachable offense—and I submit that he has committed several—is not the final determination of whether impeachment would be a good idea.
Hey, let’s pile on Christie!
Like sharks in the water, they smell blood. So there will probably be more of this sort of allegation, which seems to rest on word of mouth and involves two more officials in Christie’s administration.
And I would not be a bit surprised if some woman comes forward with sexual harassment charges soon. They are especially useful because they’re so hard to prove or disprove. In addition, no doubt teams of reporters are going through dumpsters in Christie’s vicinity even as we speak. At the very least, they might find some empty ice cream cartons.
Bridgegate was clearly true since it was substantiated by emails from the culprits themselves. Nothing has tied their actions directly to Christie, and probably nothing will. These new allegations – and whatever ones will follow – have the purpose of trying to create an atmosphere around Christie that will lead people to conclude (if they haven’t already) that of course he’s behind all of it.
That’s the way memes work. Bush is a dummy. Palin is a troglodyte Christian science-denier. Romney is an uncaring rapacious capitalist pig. Cain is a serial rapist. Christie is a corrupt bully.
My reaction? I thought threats like these were the way New Jersey politics works. I can’t imagine how, even if Christie were completely innocent (and I have no idea whether he is or isn’t), he could possibly keep this sort of thing from occurring at the hands of someone somewhere in his administration.
Of course, this is the way politics is done in Chicago, too. President Obama is part of that culture, and there is very little doubt that his administration is rife with such behavior. But hey, he doesn’t look like a corrupt bully, does he? And the MSM is playing a very different game with him than they are with Christie.
If you read just one biography of Robert Frost…
…I think it should be this one by Jay Parini.
I’ve read quite a few, and Jay Parini’s is the only one that seems to capture the Frost I sense from Frost’s poetry and his other writings. Plus, Parini’s book is very readable, with an excellent flow—something I can’t say for many of the other biographies. It reads almost like a novel.
What’s more, Parini is a poet himself and has lived most of his life in Frost country, teaching at Dartmouth in New Hampshire and Middlebury in Vermont. He understands both poetry and the territory, and he spends quite a bit of his book in fresh and insightful reading of the poems.
From a review of the book, which came out in 1999:
Robert Lee Frost, that quintessential New England writer, was born in 1874 in San Francisco. His ill-matched parents seem to have stepped from some nasty naturalist novel of the period. Frost’s mother, pretty and ”ethereal,” as Jay Parini describes her in his sturdy and well-informed new biography, ”Robert Frost: A Life,” was besotted with Swedenborg and spiritualism — her name, Belle Moodie, could hardly have been more apt. Will Frost, by contrast, was a hard-drinking, pistol-packing newspaperman who kept a jar of pickled bull’s testicles on his desk (meaning, presumably, ”Don’t mess with me”)…
Robert Frost was a brilliant student; as Parini notes, he became a better Latinist than those self-proclaimed ”classicists” Ezra Pound and T. S. Eliot. But he found academic rituals stultifying and thought the classroom was about the last place to pick up anything useful. ”We go to college,” he wrote, ”to be given one more chance to learn to read in case we haven’t learned in high school.”…
In 1958, when Frost turned 85, his publisher gave a party in his honor at the Waldorf-Astoria and invited Lionel Trilling to be the featured speaker. Trilling, who preferred cities to rural idylls, shocked everyone by confessing that he had only recently come to admire Frost’s work, specifically for its overlooked grimness. ”I regard Robert Frost as a terrifying poet,” he announced. Trilling sent a letter to Frost apologizing for the stir his remarks had caused. ”Not distressed at all,” Frost wrote back. ”You made my birthday a surprise party.” And then, in one of those swooping summations with which he regularly rewards his readers, Frost added: ”No sweeter music can come to my ears than the clash of arms over my dead body when I am down.”
Frost had a wry, playful way of speaking, so that reports of things he said or things he wrote in letters have a naturally aphoristic quality, almost like small poems themselves. And his poems have a colloquial quality, too. It all seems to be of a piece.
Trompe l’oeil

Want to know what Scott Walker thinks about it?
He tells you, here, in a long interview with John Hawkins of Right Wing News.
On Obamacare:
…[W]hat we should be doing is sharing in the frustration that most Americans have with it and then showing them that we’ve got a positive, viable alternative that’s not based on more government. It’s based on putting patients in charge, giving them the ability to purchase plans across state lines, giving them the ability to have the same tax benefits whether they buy their health insurance through their employer, whether they buy it in the market, whether they go off and do something like a health savings account. The government shouldn’t be treating them differently when it comes to tax advantages. Health care should be something that we control, not something the government controls.
…I think you’ve got to get rid of everything with Obamacare. The whole thing is a mess and I think for the handful of pundits that say, well, what about this, that, or whatever, there are little tiny components like you said, like opening up the access over state lines or things like that, that could be done ”” but I think it should be very limited and I’m not an advocate of going back to the old system. I think you repeal it and go the opposite direction. I think the old system was too bureaucratic and had too much in government intervention.
On the basic message Walker thinks Republicans should be delivering:
…[O]ne of the things that frustrates me so much in the Presidential election is I thought there was a tremendous lost opportunity ”” and obviously the clearest example of that was when Republican nominees talked about the 47% and also in a similar conversation talked about not worrying about the poor because the poor had a safety net. That really, truly doesn’t match where I’m at. I don’t think it matches with people like Ronald Reagan who was a great inspiration for me as a kid. I went back in the book and talked about how Reagan in 1980 at the National Convention in Detroit in his acceptance speech talked about things like saying if you’re living in poverty, we want to lift you out. If you’re living in despair, we want to be hope, but that hope isn’t based on more government. It’s based on empowering people with the skills and the talents and the abilities that they need to go out and control their own lives and so I think the message is really simple, I believe, and I think this was the missed opportunity. I believe the president and his allies in Washington in particular measure success in government by how many people are dependent on government, by how many people are on Medicaid, by how many people are on food stamps, by how many people are on unemployment. That’s why they want to extend unemployment benefits. They want more people signed up, more people dependent. I think we as Republicans should measure success by just the opposite ”” by how many people are no longer dependent on the government, not because we’ve got to be careful to articulate this correctly, not because we don’t care about people or because we want to push people out to the streets, but because we understand that true freedom and prosperity don’t come from the mighty hand of the government. It comes from empowering the people to control their own lives and their own destiny.
”¦.And that’s the message that we’ve got to get out to people ”” that the Left, they want you under their thumb. They want to control you. They want to control your lives. They want you to be dependent on the government. We should say we’re the ones, not only for the poor, but for young people coming out of college, for working class families, for immigrants, for others out there. We should say we are the ones who empower the American Dream. We’re the ones who say you can do and be anything you want, but it’s because we empower you with the ability and the platform to do that. Then it’s up to you to make that happen. The other side tells you they want to help you, but in the end they want to keep you limited in how far you can grow.
I think that last paragraph might be the more important part. It’s hard for politicians not to sound as though they’re just saying the same-old same-old blah blah blah. I’m not the best judge of how political rhetoric comes across—when most politicians (on either side) speak, my reaction alternates between a cringe and a yawn. Ordinarily, for me the difference between a Republican speaker and a Democratic speaker is merely the cringe/yawn ratio, and I usually can’t take too much of either.
The things I like about Walker (my front-runner so far) are his executive experience, his principles, and his guts and fighting spirit, as well as his success in a mostly-blue state such as Wisconsin countering whatever the left could throw at him. That is a formidable accomplishment.
His rhetoric and charisma, I suspect, leave quite a bit to be desired. But I don’t know how much they are lacking because I haven’t watched or listened to him speak all that much. I fear Walker will have too much of the blah-blah-blah factor, but I don’t know; that last paragraph I quoted above seems to have a good ring to it.
What do I like about Christie (and yes, as I’ve written before, if he’s nominated I most definitely plan to vote for him—unless some new and truly abominable revelation comes out)? His executive experience, his guts and fighting spirit, and his success in a blue state such as New Jersey. Note what I left out from the Walker list: his conservative principles. I do think Christie has some, at least in fiscal matters.
But the one thing Christie’s got that Walker doesn’t have is the fact that when Christie speaks he minimizes both the boring factor and the cringe factor, at least for me. Perhaps I’m partial to his manner because it speaks to me of home. It’s very very familiar to me because it conjures up the people who surrounded me where I was growing up (not my family especially, but the larger community where I was raised). I recognize it and think I understand it. The style has energy, humor, and bluntness, and I find that refreshing in a politician.
I don’t know how many people agree with me, though. I’m not exactly typical of voters, or even of Republican or conservative voters. Nor, probably, are you.
[ADDENDUM: I just noticed that Ann Althouse highlighted that same paragraph I did from Walker’s interview. That’s interesting, since Althouse voted for Obama in 2008. She writes:
That’s a nice combination of staunch conservatism with empathy and caring, which is, I think, what the GOP should want in its next presidential candidate. Walker has absorbed and processed the “income inequality” theme that the Democratic Party has chosen to push.
Agreed.]
[ADDENDUM II: Ace weighs in, too.]
Obama announces new NSA policy—sort of
Actually (and I didn’t listen to his speech) it appears that he asked Congress to study the situation and make recommendations by the end of March as to how the phone metadata program can work to collect the information without that data being stored by the government. Andrew McCarthy adds:
Expect delay on this, with the tough calls punted to Congress. It is entirely appropriate that this should be settled by legislation, but the controversy will still center on how the executive branch ”“ which has independent constitutional authority to conduct surveillance for foreign intelligence purposes ”“ exploits whatever Congress designs.
It’s interesting that Obama is saying to Congress, “You figure it out.” And then, as McCarthy suggests, he’ll do whatever he wants?
“Wolf of Wall Street” fashion
And now for a change of pace—I guess they still call it “fashion.”
These outfits were seen at the UK premiere of the Scorcese film “The Wolf of Wall Street.” I am in awe at the almost infinite variety of their deep horribleness, although some are clearly more horrible than others.
This woman was putting on her underwear, then unfortunately got tangled in a sooty cobweb. Pressed for time, she decided to throw on her boyfriend’s jacket and hoped it would cover the whole thing. It didn’t:

This woman’s inspiration: flying squirrel? Bat? Zorro?

This woman had the same initial problem as the one in the first photo, except instead of throwing on her boyfriend’s jacket, she decided to go with her very own flesh-colored bathrobe:

This lady is attempting the French schoolgirl look, a la Leslie Caron in “Gigi,” but doesn’t quite make the grade (although she is by far the best of the lot):

Why? WHY? Any of these women could wear nearly anything and look better than this.
In case you’re wondering about Leslie Caron and that French schoolgirl look, this is what I mean:


Caron—an absolute charmer.