Almost twenty years ago I hurt my back and sustained injuries to both arms that left me with what’s known as neuropathic pain.
We all know what pain from an injury feels like. But if you’re fortunate, you don’t know—and will never have to learn from personal experience—what neuropathic pain is like.
Nerves ordinarily conduct pain impulses when tissues are damaged, but that sort of pain corresponds to the degree of injury and is time-limited. Once healing occurs, the pain (or almost all of it) goes away. Neuropathic pain is different; it arises from injury to the nerves themselves. They become disordered in a host of ways, and the quality of the pain impulses is quite different from that of the more familiar types of pain, and has a marked tendency to become chronic:
Neuropathic pain, in contrast to nociceptive pain, is described as “burning”, “electric”, “tingling”, and “shooting” in nature. It can be continuous or paroxysmal in presentation.
Not that much is known about nerve pain today, and it remains exceedingly difficult to treat. But about twenty years ago, when I began to deal with it myself, it was the relative Dark Ages of pain control.
When I hurt my arms it was terrifying; the pain felt like nothing I’d ever had before, and it was with me 24/7. The best I can do to describe it is to say that among its many horrific qualities was the feeling of having sustained a severe sunburn on the entire surface of both arms. But with a real sunburn, there are salves and ointments to apply, you know why you’re hurting, and you know that in a few days the pain will go away.
This pain was different. It waxed and waned in odd and erratic fashion, although it tended to be at its worst at night, which made sleep nearly impossible and the nights a long drawn-out torment. It wasn’t just the burning, either. There was also tingling and stabbing pain and severe achiness and exquisite sensitivity and weakness and pressure and all sorts of odd sensations that gave me the feeling that my body had become a sadistic trickster bent on driving me mad.
I’m grateful that no doctor ever suggested my pain was imaginary or psychogenic in nature. It was clear to them from my history and findings that I had sustained nerve injuries in both arms. Several nerves were affected, but by far the most severe symptoms were in the ulnar nerves:
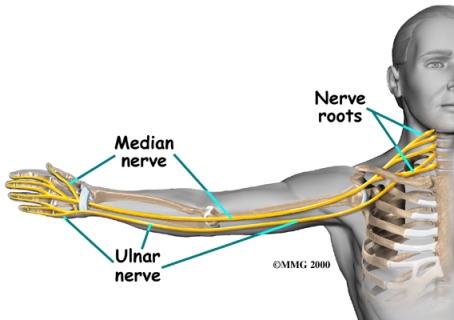
The first doctor I saw was an arm specialist, and he sent me to a neurologist for tests called EMGs that measure nerve conductivity and attempt to pinpoint the site and extent of the damage. My results were ambiguous: conductivity was slowed, especially across the elbow, but not enough to indicate a need for surgery, and not enough to show which of several different types of surgery I should have (if you look at the diagram above you’ll see that there are a number of possible areas for compression of the ulnar nerve, and the site determines the type of surgery indicated).
When my doctor told me the news, he sent me home after saying that he could do nothing for me. I still remember his chilling words, “Even morphine won’t touch this sort of pain.”
It turned out he was wrong about that; morphine will touch it, but only a little. In fact, methadone tends to touch it a lot more firmly. But I wasn’t seeking drugs, especially opioids, which have a host of dangerous side effects; I was seeking a way to heal.
Over the years I tried many things, to little or no lasting effect. Several types of non-opioid medication. Many different sorts of physical therapy, too numerous to count. Cortisone. Experimental MRIs that were supposed to image damaged nerves. I also sunk many thousands of dollars into the alternative medicine industry. Acupuncture. Osteopathy. Homeopathy. Naturopathy. Reiki. Magnets. And more. Along the way I met many good people and many charlatans, the kind and the cruel, the caring and the indifferent.
And after a while I went to the experts. Since my case was somewhat unusual and some of the various syndromes under consideration somewhat rare, there weren’t a lot of knowledgeable people and the ones who did exist were spread out around the country. I don’t remember exactly how many I consulted—quite a few in Boston, for example—but to find the most expert of experts I had to do a lot of research and travel quite a distance.
My insurance covered much of this, except for the alternative practitioners. I had always had a horror of not having medical choices, so for years my husband and I had paid extra to have the freedom to go to other states, and not to be bound by a primary care physician’s recommendations and restrictions.
It was money well spent. But I soon discovered that even the experts disagreed as to what the best treatment would be. One wanted me to have a very invasive and dangerous surgery to remove my first rib through my armpit. One thought I should have a scalene muscle in my neck removed as well. Each thought the surgery would probably help somewhat, but they told me the risk of complications and permanent damage was high, and the chances of marked improvement not good.
There was a also a somewhat less risky (although still chancy) elbow surgery I could have (actually, I had a choice among at least three types of elbow surgery). But the doctors in Boston and the East refused to perform it on me because, although my symptoms pointed to ulnar nerve entrapment at the elbow, the findings on my EMG tests (which had been repeated about five times over the years) remained ambiguous.
Finally, nine years into this, facing continual debilitating and demoralizing pain, and having exhausted all the non-surgical remedies I could find, I went with my gut and made my decision. My perception was that the bulk of my pain originated in the elbow area. If doctors in the East wouldn’t operate on my elbow (the right, which was worse than the left), there was a famous doctor in the West who would. He was one of the world’s experts in elbows and had done more surgery of this type than almost any other surgeon in the world. He took a careful history, looked at all my tests, and examined me thoroughly. He announced himself willing to perform the surgery to release my ulnar nerve from the elbow and move it to a new place under a muscle in my forearm.
Before the surgery I was given a sheet full of dire warnings for me to sign. I knew that most other doctors would have disagreed with this man’s decision. I had no idea whether I was doing the right thing, and he gave me no guarantees whatsoever, except that he would do his best. But I knew I had run out of alternatives and that I could not live with myself if I didn’t try for what now appeared to be my best (and perhaps only) hope of getting better. I also knew I would probably never be normal, but I’d almost forgotten what that was; I’d settle for “improved.” So I was at peace with my decision.
I remained at peace with it throughout my lengthy and extremely difficult recuperation, lasting about two years.
In the recovery room right after the surgery, the two doctors who’d operated on me had a fascinating but sobering tale to tell: they were surprised at the amount of damage they’d found in my elbow, much worse than expected. My ulnar nerve itself was red and swollen. There was at least an inch of thick scar tissue pinning it down completely within the cubital tunnel, the passageway in the elbow through which the ulnar nerve normally runs, so that in my case the nerve was unable to move freely. This is what had caused at least some of the terrible pressure and pain; every time I’d moved my arm I was stretching and injuring the nerve.
The doctors added that the surgery had taken twice as long as normal, and had traumatized the nerve much more than usual. They also had noticed that other smaller nerves had gotten tangled up in the mess of scar tissue, and they’d had no recourse but to cut those nerves as well. They could not predict what the effects of that severing would be.
The doctors made it clear that they did not know how well I’d recover, or how long it would take. We were in uncharted waters. But I knew I’d gone to the best people possible. And they told me something else that I took to heart during the many dark hours that followed: it seemed I’d had the correct surgery, after all. Although they could not guarantee that I would improve, the damage they had viewed when they had opened up my arm was so bad that they could not see how I ever could have improved without an operation.
Now I’m grateful every day that I had that surgery. Although it took a couple of years to recover, I would say I’ve improved about 75% as a result of the operation. That means, quite simply, that I got my life back. Not a completely normal life—but I wasn’t really expecting that. It’s a life that, although I still have to be protective and careful, allows me to do so many things I couldn’t do before, and to do them without significant pain or the need to take powerful medications.
Why am I telling this long and tedious and rather personal tale? Although all these years have passed, I’ve thought of it recently in connection with the health care reforms being discussed in Washington. The flexibility of my insurance coverage was one of the main reasons I was able to go so far in seeking relief; without it I have little doubt that I’d still be be in terrible trouble.
It was actually my injuries that first propelled me online over ten years ago, looking for information to help me with my decisions, and to read about the experiences of other people who suffered from similar problems. One of the things I found at that time that made a deep impression on me were the stories told by patients in Canada and Britain. Although they didn’t have to worry about insurance coverage, they were uniformly the most miserable of all the chronic pain patients on several message boards I frequented. They had to wait forever for tests. There were far fewer specialists in Canada and Britain who knew anything about their injuries or how to treat them either surgically or medically. The problems of these patients were generally considered unimportant and they were given low priority.
Until that time, if I’d thought about the health care system in those countries at all, I had assumed it was a great thing that there was universal coverage. But during this experience I learned that, at least for nerve injuries and chronic pain of the sort I had, the care here was far better. In fact, many of these people dreamed of saving up enough money to come to the US to some of the surgeons I’d been able to see. But they could not afford it, and they continued to suffer.
I’m not a rich person. But ever since then I’ve continued to pay extra for the medical insurance most likely to preserve my freedom to choose. If I hadn’t been able to have surgery on the west coast, I believe that even now, ten years later, I would probably be suffering from pain at or above the level of those early years. The prospect is so dreadful that I shudder to even think about it. I’m just grateful that wasn’t the case.
My back injury had a different course. I still have some pain and vulnerability there but I’ve never had surgery, because I got major relief from an epidural steroid injection I received about fifteen years ago. That’s probably why this article about a newly-announced British policy towards those very same injections caught my eye:
The Government’s drug rationing watchdog says “therapeutic” injections of steroids, such as cortisone, which are used to reduce inflammation, should no longer be offered to patients suffering from persistent lower back pain when the cause is not known.
Instead the National Institute of Health and Clinical Excellence (NICE) is ordering doctors to offer patients remedies like acupuncture and osteopathy…
The NHS currently issues more than 60,000 treatments of steroid injections every year. NICE said in its guidance it wants to cut this to just 3,000 treatments a year, a move which would save the NHS £33 million.
That’s a proposed 95% reduction in the number of these injections, which are an invaluable aid to the treatment of back injury—which, by the way, is an area of medicine for which “the cause” is rarely known. As the article goes on to point out, such treatments are a relatively simple and less risky way of saving many people from being on opioids for the rest of their lives, or having much more expensive and risky surgery in the future. Penny wise and pound foolish.
And perhaps a portent of things to come here.