Here’s an article purporting to explain why South Korea is doing relatively well against COVID-19:
Behind its success so far has been the most expansive and well-organized testing program in the world, combined with extensive efforts to isolate infected people and trace and quarantine their contacts. South Korea has tested more than 270,000 people, which amounts to more than 5200 tests per million inhabitants—more than any other country except tiny Bahrain, according to the Worldometer website. The United States has so far carried out 74 tests per 1 million inhabitants, data from the U.S. Centers for Disease Control and Prevention show.
But a caveat:
Yet whether the success will hold is unclear. New case numbers are declining largely because the herculean effort to investigate a massive cluster of more than 5000 cases—60% of the nation’s total—linked to the Shincheonji Church of Jesus, a secretive, messianic megachurch, is winding down. But because of that effort, “We have not looked hard in other parts of Korea,” says Oh Myoung-Don, an infectious disease specialist at Seoul National University.
New clusters are now appearing. Since last week, authorities have reported 129 new infections, most linked to a Seoul call center. “This could be the initiation of community spread,” through Seoul and its surrounding Gyeonggi province, Kim says.
So it may just be a lull, and a function of the particularly localized pattern of infection in Korea as well as the country’s mitigation efforts. We don’t know what factors are causing what effect, at least I’ve not read anything that indicates an answer.
Testing may have been especially helpful in Korea because of that initial geographic and social localization:
The surge initially overwhelmed testing capabilities and KCDC’s 130 disease detectives couldn’t keep up, Kim says. Contact tracing efforts were concentrated on the Shincheonji cluster, in which 80% of those reporting respiratory symptoms proved positive, compared with only 10% in other clusters.
I would wager that most people who read this article come away convinced that South Korea’s aggressive testing approach has made all the difference, and the US has been negligent in not testing an equivalent number of people. I agree that the glitches in the development of the US testing kits – a manufacturing error, and then slowness involving bureaucratic red tape that needed cutting – has hampered our efforts. But has it actually made all that big a difference?
For some reason – and I think it may be the early travel restrictions put in place here – the US actually has a pretty good record compared to South Korea in term of severe cases and deaths. Take a look at this chart for today, the one entitled “Confirmed Cases and Deaths by Country, Territory, or Conveyance.” It has some interesting columns, such as “active cases,” “serious, critical cases,” “total deaths,” and “new deaths,” country by country. Since all the countries involved have different populations, it has another interesting column entitled “total cases per 1 million population.”
At the moment, here are the figures for South Korea: 6789 active cases, 59 cases currently in serious or critical condition, 3 new deaths, and 84 total deaths so far out of 8413 total cases since it all began. That means that in South Korea, the number of cases per million so far has been 164, and the deaths have involved .000001632% of the population.
In the US, we have had 7708 confirmed cases so far (with much less testing, so perhaps the rates are much much higher, perhaps just slightly higher, or perhaps in-between). Our numbers are still in the climbing stage, with 1297 new cases, a total of 120 deaths, and 11 new deaths. But of the 7482 currently active cases in the US, only 12 are considered serious or critical. That’s so low that I wonder whether it’s a typo, but if it’s not it’s pretty extraordinary, and it’s much lower than Korea’s already low ratio of serious cases to active cases.
In addition, because the USA has about seven times more people than South Korea, our deaths have so far involved .0000003667 of our population. That’s a very much smaller figure than in South Korea (we also have 23 diagnosed cases per million people, only about about 14% of South Korea’s figure, although that’s almost certainly because we just haven’t tested all that many people, so I don’t place much importance on the comparison).
It’s the death figures that have gotten my attention. Why is our death rate expressed as a percentage of the total population so much lower? Is it just that we haven’t peaked, and South Korea has? Or is something else going on?
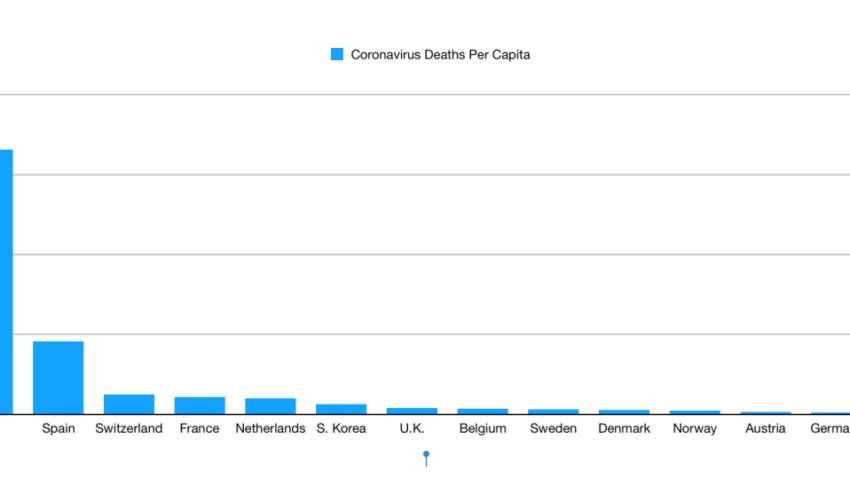
For that matter, why is our death rate per million also so much lower than that of European countries? (From Powerline):
Again, these are just the figures as of today, and we could experience a huge surge. But (and I can’t find the link for this right now, although I remember reading it) our caseload began about the same time as South Korea’s.
My guess is that Trump’s much-maligned restrictions on travel from China, put into place on January 31, when there were only seven diagnosed cases in the US, made a significant part of the difference. The press, the Democrats, the left, and the NeverTrumpers were up in arms about that racist xenophobe Trump. And yet his action – as well as later restrictions on Iran and then on February 29 his adding restrictions on Italy and South Korea – seems very smart, particularly the early restriction regarding China.
The press and the Democrats have invested a lot in conveying to the American people that Trump is both a loose cannon and a racist. So when he does something the rest of the world isn’t doing, and it restricts travel from a certain country, it’s a no-brainer for them to scream “racist!,” and they convince much of America that it’s the case. Now they would like you to conveniently forget that Trump’s action was based on the idea of limiting the importation of a disease early on in order to delay its spread as much as possible in order to give the country and the health care system time to prepare, and that it probably accounts for the fact that the death rate in this country is lower than in most of the rest of the world – so far.
[NOTE: Another factor is that South Korea has supposedly had a lot of success treating patients with the antimalaria drug Chloroquine, a widely available medication that has been used in this country for ages for many things, and which is also cheap. And yet it also appears that the FDA has been setting up roadblocks on its use for COVID-19 in this country. Why, if it’s already been in use and approved and considered very safe? I’d like to hear a lot more about that. I understand that they must test it and make sure it works, but why not allow it to be used in very serious cases only, and have a big push to test it ASAP?]
